
 One of the most common health complaints today is the experience of fatigue and lethargy. If you have fatigue along with other symptoms such as difficulty concentrating, insomnia, inability to lose weight, feeling anxious, allergies, or brain fog, Adrenal Fatigue may be at the root of the problem.
One of the most common health complaints today is the experience of fatigue and lethargy. If you have fatigue along with other symptoms such as difficulty concentrating, insomnia, inability to lose weight, feeling anxious, allergies, or brain fog, Adrenal Fatigue may be at the root of the problem.
Adrenal Fatigue, or hypoadrenia, is used to describe a collection of nonspecific symptoms, such as fatigue, body aches, nervousness, sleep disturbances, brain fog, and sugar or salt cravings, which emerge under conditions of prolonged stress. Stress triggers the activation of the hypothalamic-pituitary-adrenal (HPA) axis, prompting your adrenal glands to release cortisol and other hormones to combat the stress. However, if stress persists over time, the demand for cortisol overwhelms the adrenals, leading to insufficient cortisol production. This marks the onset of Adrenal Fatigue or Adrenal Fatigue Syndrome (AFS). Initially, symptoms may be subtle but worsen in intensity and impact as prolonged stress persists. We will be using the terms Adrenal Fatigue Syndrome and Adrenal Fatigue interchangeably because Adrenal Fatigue is the most commonly used terminology recognized and used by the public. The term "syndrome" just means there is a cluster of symptoms that adrenal fatigue is associated with.
Adrenal Fatigue is not a medical condition recognized by mainstream institutions because the adrenal glands are structurally normal and low cortisol, the most common associated finding, could be caused by factors outside the adrenal glands. While the medical community largely does not recognize adrenal fatigue as a legitimate medical condition, the symptoms are undeniably significant to those who suffer from them.
People think of Adrenal Fatigue (also called Adrenal Fatigue Syndrome, or AFS) as a condition related to stress. Thus, the solution in conventional medicine is to tell the person to "relax" or take anti-depressants or thyroid medications as a band-aid approach to improving energy. This does not solve the underlying issue and over time, the condition could worsen as the root cause is not addressed.
Our body has built-in mechanisms to deal with prolonged stress. The control center to handling stress is the adrenal glands. It's important to look at the Adrenal Fatigue from a comprehensive neuroendocrine and metabolic standpoint in order to fully address all the symptoms that arise.
Do not confuse Adrenal Fatigue with another medical condition called Addison's disease. Addison's disease has adrenal glands that are not functioning according to conventional endocrinologists' standards. Addison's disease is often caused by an auto-immune dysfunction. Adrenal Fatigue is caused by stress or other factors. These can include dysregulation of the HPA axis, nervous system problems, immune system problems, and metabolic-nutritional problems. It is a complex condition with complex clinical presentation, depending on the stage of dysfunction. Those in neuroscience may prefer to label this condition Hypothalamic-Pituitary-Adrenal (HPA) Axis Dysregulation. This is due to the strong association with dysfunction of the HPA axis. A forward-looking endocrinologist may be more comfortable with calling this condition Non-Adrenal Illness Affecting Adrenal Function because of the associated low cortisol output which does not meet the diagnostic criteria for Adrenal Insufficiency.
Conventional medicine only recognizes Addison's disease as hypoadrenia. As such, it is not surprising if your doctor is unfamiliar with this condition. Adrenal Fatigue Syndrome is a sub-clinical non-Addison's form of adrenal dysfunction. Because there are many causes, Adrenal Fatigue Syndrome is a more accurate name. The addition of "syndrome" implies no definitive cause. It would be up to the physician to determine the list of symptoms and signs appropriate to the syndrome.
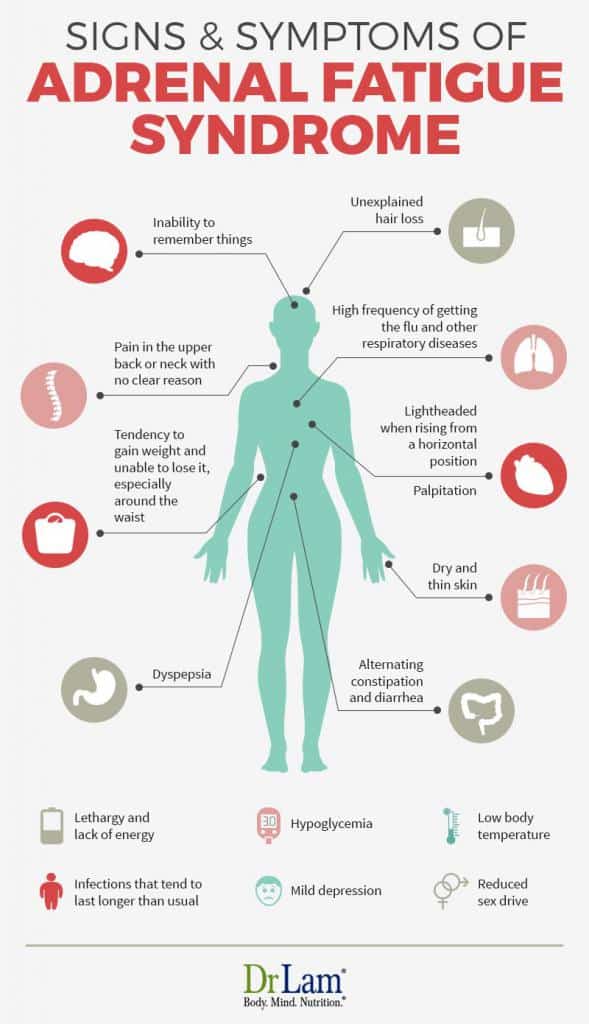
 Symptoms can vary from person to person and the severity of individual symptoms can also vary as the condition progresses. Here’s a list of the most common symptoms among people with AFS.
Symptoms can vary from person to person and the severity of individual symptoms can also vary as the condition progresses. Here’s a list of the most common symptoms among people with AFS.
If you have many of these signs and symptoms, it is time to consider Adrenal Fatigue as a possible cause. None of the signs or symptoms by themselves can definitively pinpoint Adrenal Fatigue. However, when looked at collectively, these signs and symptoms form a specific picture of a person under stress. These signs and symptoms are often the end result of acute, severe, chronic, or excessive stress. The body is unable to reduce such stress.
The ability to handle stress, physical or emotional, is a cornerstone to human survival. Our body has a stress modulation system in place, known as the neuroendometabolic (NEM) stress response. The adrenal glands are part of this response system. When these glands become dysfunctional, our body's ability to handle stress is reduced.
» Infographic: More Signs and Symptoms of Adrenal Fatigue
The adrenal glands are two small glands, each about the size of a large grape. They are on top of the kidneys. Their purpose is to help the body cope with stress and help it to survive. Each adrenal gland has two compartments. The inner compartment is the adrenal medulla. The adrenal medulla modulates the sympathetic nervous system through secretion and regulation of two hormones called epinephrine and norepinephrine. Epinephrine and norepinephrine are responsible for the fight or flight response.
The outer compartment is the adrenal cortex. The adrenal cortex comprises 80 percent of the adrenal gland and produces over 50 different hormones. These hormones make up three major classes: glucocorticoids, mineralocorticoids and sex hormones.
The most important glucocorticoid is cortisol. When cortisol is lowered, the body will be unable to deal with stress. This happens in Adrenal Fatigue.
Mineralocorticoids modulate the delicate balance of minerals in the cell, especially sodium and potassium. An example is aldosterone. It thus regulates our blood pressure and the fluid in the body. Stress increases the release of aldosterone, causing sodium retention. This results in water retention and high blood pressure. Potassium and magnesium are lost in the early stages of Adrenal Fatigue. Magnesium is involved in over 300 enzymatic reactions in the body. When the body lacks magnesium, cardiac arrhythmias and other symptoms may arise.
The adrenal cortex is also responsible for producing all the sex hormones, although in small amounts. One exception is DHEA, a weak androgenic hormone that is made in large amounts in both sexes. DHEA, together with testosterone and estrogen, are made from pregnenolone. Pregnenolone also leads to the production of progesterone. It is one of the intermediary steps in the making of cortisol. A prolonged deficiency in pregnenolone will lead to reduced glucocorticosteroids and mineralocorticoids. This can occur in Adrenal Fatigue in a phenomenon called pregnenolone steal, where the adrenals utilize resources to produce more cortisol and therefore less pregnenolone is available.
When stressed, the body reacts by mounting a stress response. The body's stress response is also known as the NeuroEndoMetbolic stress response system. It contains 6 circuits that help to regulate stress: hormone, bioenergetic, detoxification, inflammatory, neuroaffective, and cardionomic. Each of the circuits is regulated by a different set of organs of systems in the body. These 6 different circuits help to regulate the stress in the body, however, if stress is chronic, then symptoms may start to arise as different circuits and their respective organs become dysregulated. It stimulates the sympathetic nervous system. This is also called the "fight or flight" response as the body arms itself to face what it perceives as a danger. The adrenal medulla secretes epinephrine. The HPA axis also releases ACTH, which causes the adrenal cortex to increase production of cortisol.
The most important anti-stress hormone in the body is cortisol. Cortisol protects the body from excessive Adrenal Fatigue through:
Cortisol increases blood sugar levels in the body. Cortisol works in tandem with insulin from the pancreas to provide adequate glucose to the cells for energy. More energy is needed when the body is under stress, from any source, and cortisol is the hormone that makes this happen. In Adrenal Fatigue, more cortisol is secreted during the early stages. In the later stages of Adrenal Fatigue (when the adrenal glands become exhausted), cortisol output is reduced.
Cortisol is a powerful anti-inflammatory agent. When we have a minor injury or a muscle strain, our body's inflammatory cascade is initiated. Cortisol is secreted as part of the anti-inflammatory response. Its goal is to remove and prevent swelling and redness of tissues. These anti-inflammatory responses prevent mosquito bites from enlarging, bronchial stress, and eyes from swelling shut from allergies.
People with high cortisol levels are much weaker from the immunological point of view. Cortisol influences most cells that take part in the immune reaction, especially white blood cells. Cortisol suppresses white blood cells, natural killer cells, monocytes, macrophages, and mast cells. It also suppresses Adrenal Fatigue.
Cortisol contracts mid-size arteries. People with low cortisol have low blood pressure. They do not respond to other body agents that constrict blood vessels. Cortisol tends to increase blood pressure.
People with Adrenal Fatigue cannot tolerate stress and succumb to severe stress. Higher stress levels require higher levels of cortisol. When the cortisol level cannot rise in response to stress, it is impossible to maintain the body in optimum stress response.
Cortisol sustains life via two opposite, but related, kinds of regulatory actions. It releases and activates the existing defense mechanisms of the body. At the same time, it shuts down and modifies the same mechanisms to prevent them.
The hypothalamus-pituitary-adrenal (HPA) axis controls the adrenal glands. There is an existing negative feedback loop that governs the amount of adrenal hormones secreted under normal circumstances. For example, the HPA axis adjusts cortisol levels according to the body's need via a hormone called Adrenal Corticotropic Hormone (ACTH). The pituitary gland secretes ACTH in response to signals from the hypothalamus. When the ACTH binds to the walls of the adrenal cells, a chain reaction occurs within the cell. The adrenal cells release cholesterol. Cholesterol is then converted to pregnenolone, the first hormone in the adrenal cascade. After this, cortisol is released into the blood stream. It travels in the circulatory system to all parts of the body and back to the hypothalamus.
Cortisol and ACTH are not secreted uniformly throughout the day. They follow a diurnal pattern. The highest level secreted at around 8:00 a.m. in the morning. Cortisol then start to decline throughout the day. Episodic spikes during the day can also occur when the body is stressed. Certain foods can elevate cortisol as well. The cortisol level is at its lowest between midnight and 4:00 a.m.
Chronic stress is common in Western society. AFS can occur when the amount of stress exceeds the body’s capacity to compensate and recover.
Unfortunately, life itself can be stressful. At any one time, you could be facing a number of situations that cause stress, from work pressures and job changes to illnesses, marital problems, or environment changes. Pain, physical illnesses, and chronic health problems can also cause physical stress on the body.
 Chronic stress is common in western society. The most common causes of stress are work pressure, changing jobs, death of a loved one, moving homes, illness, and marital disruption. Adrenal Fatigue occurs when the amount of stress exceeds the capacity of the body to compensate and recover.
Chronic stress is common in western society. The most common causes of stress are work pressure, changing jobs, death of a loved one, moving homes, illness, and marital disruption. Adrenal Fatigue occurs when the amount of stress exceeds the capacity of the body to compensate and recover.
One of the most overlooked causes of Adrenal Fatigue is chronic or severe infection. This gives rise to an inflammatory response. Such infection can occur sub-clinically with no obvious signs at all. Parasitic and bacterial infections including Giardia and H. pylori are often the main causes.
Adrenal weakness progresses through stages as the body de-compensates. It is the body's strategy to return to a state of simplicity from a life that is too complex for the body to handle.
In this stage, the body is alarmed by the stressors and mounts an aggressive anti-stress response to reduce stress levels. Some doctors call this the Early Fatigue stage.
ACTH increases from the pituitary gland. The adrenals are stimulated to mount a retaliation response. epinephrine and cortisol are released. There is usually, but not always, a corresponding reduction in the DHEA production. No symptoms are reported at this stage. There may be a sense of being tired. Daily activities continue unaffected.
With under chronic or severe stress, the adrenals eventually are unable to keep up with the body's demand for cortisol. Cortisol output will start to decline from a high level back to a normal level, while ACTH remains high. The adrenals start to become exhausted. Morning, noon, or afternoon cortisol levels are often low. Nighttime cortisol level is usually normal. Anxiety starts to set in, and the person becomes irritable. Insomnia becomes more common, as it takes longer to fall asleep. There are also frequent awakenings as well. Infections can become recurrent. PMS and menstrual irregularities surface. Symptoms suggestive of hypothyroidism (such as a sensation of feeling cold along with a sluggish metabolism) become prevalent.
A phenomenon called pregnenolone steal (also called cortisol shunt) sets in. The body starts to favor cortisol production over other hormones. Other hormones such as pregnenolone, DHEA, testosterone, and estrogen are less favored and start to decline. As a result, total pregnenolone output is reduced but the total cortisol output continues at a normal level. The daily diurnal cycle of cortisol shows a dysfunctional pattern. Cortisol is low in the morning, when it is needed the most. Nighttime cortisol is usually still normal.
There is occasional mild fatigue. A nap or some time off work usually can help the recovery process greatly.
Despite rising ACTH, the adrenals cannot keep up with the body's demand for cortisol. This may happen over a few years. Total cortisol output is reduced, and DHEA falls far below average. The nighttime cortisol level is usually reduced as the HPA axis "crash". The body is unable to maintain homeostasis. Early in this stage, mild symptoms characteristic of the first and second stages of Adrenal Fatigue become persistent or chronic (Phase A). As the condition gets worse, multiple endocrine axis imbalances tend to occur (Phase B). This manifests in the form of ovarian-adrenal-thyroid (OAT) axis imbalance in females and adrenal-thyroid axis imbalance in males. The body is in a constant state of mild to moderate fatigue in phase A and B.
As the body continues its downward path of impaired function, it gathers steam. The body becomes compromised in trying to maintain the fine controls of homeostasis. Normal equilibrium is lost. The body enters a state of reactive disequilibrium (Phase C). Severe fatigue is the norm for those with Phase C.
Your body will try to maintain equilibrium with the activation of the autonomic nervous system (ANS). However, the body is too fatigued. Other pathways of the NEM stress response are damaged as well. impaired metabolic, clearance, and detoxification pathways give rise to paradoxical, unpredictable, and exaggerated outcomes. Reactive sugar imbalances, fragile blood pressure, postural hypotension, heart palpitations, POTS, dizziness, anxiety reactions, being "wired and tired," periodic adrenaline rushes, fragile fluid state; such as hypersensitive dilutional hyponatremia, sudden onset of anxiety, and a sensation of impending doom are common.
There is a strong mind-body connection. Every thought process invokes a physiological response. Many of these symptoms represent what a "reactive sympathoadrenal response." This response is the result of an over-activation of two components of the ANS - the sympathetic nervous system (SNS) and the adrenomedullary hormonal system (AHS). These two components constitute the sympathoadrenal system (SAS). the body bathes in a sea of epinephrine and norepinephrine, when the SAS is over-activated due to stress. These two hormones are responsible for many of the above-mentioned symptoms.
As the body's key hormones fall below the minimum required reserve for normal function and output fails, the body may down-regulate the amount needed to preserve what is on hand for only the most essential body functions. This near-failure state (Phase D) is quite serious and requires professional attention. This is a state of extreme low energy as the body tries to conserve to survive. Normally helpful nutrients may backfire with paradoxical responses being the hallmark. Those in Phase D are usually bedridden most of the time. Normal daily chores need ambulatory help. Traditional macro-nutritional approaches may be helpful. But, the body may continue to decompensate. In these cases, a carefully titrated micro-nutritional program may be necessary to help the restore the body.
Eventually, the adrenals are totally exhausted. In this stage, the line between Adrenal Fatigue and clinical Addison's disease can be blurry.
Typical symptoms of Addison's disease may start to emerge. Fatigue becomes extreme. Other symptoms include weight loss, muscle weakness, loss of appetite, nausea, vomiting, hypoglycemia, headache, sweating, irregular menstrual cycles, depression, orthostatic hypotension, dehydration, and electrolyte imbalances. The body appears to have lost its normal homeostasis and is breaking down. If not attended to, the natural progression of this condition may be fatal.
The following diagram shows how Adrenal Fatigue progresses with time through the stages. This is not for diagnosis purposes. Adrenal Fatigue is not a recognized medical condition by mainstream institutions. This diagram helps to paint a broad picture of what is seen clinically. Each person's progression varies tremendously and is dependent on a wide variety of factors.
Adrenal Fatigue has been recognized as a distinct clinical syndrome since the turn of the 20th century. But, most doctors are unfamiliar with this condition. That is because it is difficult to diagnose by traditional blood tests. Normal blood tests detect severe, changes in adrenal hormones, such as Addison's Disease. However, Addison's disease afflicts only 4 out of 100,000 and is often the result of an autoimmune disease or infectious origin. Blood tests are also useful to detect extreme, excessive levels of cortisol, a condition known as Cushing's disease.
Let's examine this in more detail. The ACTH (adrenocorticotropic hormone) challenge test is the conventional test used. This test recognizes extreme underproduction or overproduction of hormone levels. It measures the top and bottom 2 percent of a bell curve. In other words, makingf a diagnosis requires adrenal function to be very low (the bottom 2 percent).
 Symptoms of non-Addison adrenal fatigue, meanwhile, can start to present itself after a 15 percent deviation from the mean on the bell curve. Therefore, the adrenal glands could be functioning anywhere from 15 to 48 percent below the norm and not be detected by the ACTH test.
Symptoms of non-Addison adrenal fatigue, meanwhile, can start to present itself after a 15 percent deviation from the mean on the bell curve. Therefore, the adrenal glands could be functioning anywhere from 15 to 48 percent below the norm and not be detected by the ACTH test.
Adrenal hormones are low in the case of Adrenal Fatigue. But they are still within the "normal" range and not low enough to warrant the diagnosis of Addison's disease. Such "normal" levels of cortisol and ACTH do not mean that the patient is free from adrenal malfunction. Conventional doctors are not taught the significance of sub-clinical Addison's disease, or Non-Addison's Hypoadrenia (commonly referred to as Adrenal Fatigue). Blood tests misguide them. As a result, patients tested for adrenal functions are told they are "normal". But in reality, their adrenal glands are performing sub-optimally, with clear signs and symptoms as the body cries out for help and attention.
Cortisol levels are crucial indicators of adrenal health and can be assessed through various tests, including blood, urine, or saliva. Home saliva cortisol and hormone testing kits for adrenal fatigue are designed to identify cortisol imbalances by requiring the user to collect multiple samples over a whole day. This method provides a comprehensive view of the body's stress response throughout the day. Although dry urine samples are another option for evaluating cortisol levels, their accuracy in assessing stress response is not widely supported by clinical research. Additionally, measuring salivary DHEA in conjunction with cortisol can also indicate adrenal gland function.
Monitoring cortisol at different times—morning, lunch, mid-afternoon, and evening—helps correlate cortisol levels with potential adrenal issues, such as metabolic imbalances or baseline adrenal function. It’s essential to align these cortisol measurements with specific symptoms experienced throughout the day to get a clearer picture of adrenal health.
However, given the significant individual differences and the dynamic nature of the body, laboratory tests should be used thoughtfully and only when necessary to ensure cost-effectiveness and relevance. It's not unusual for individuals with adrenal fatigue symptoms to have normal lab results and vice versa. In cases of advanced adrenal fatigue, the 4 point saliva cortisol curve often becomes flattened, which can persist during recovery, leading to potentially confusing test results. Depending on tests alone can be a common mistake in managing adrenal fatigue.
A thorough history taken by an experienced provider or nutritional health coach remains the most effective method to determine adrenal fatigue status, surpassing any lab test. Laboratory tests should be utilized as supplementary tools, rather than the primary measure of adrenal function and recovery decisions. To effectively address symptoms attributed to adrenal fatigue, it is vital to conduct medical tests to exclude conditions like Addison's disease. The ACTH stimulation test is one method used to assess the adrenal glands' cortisol production in response to ACTH and can rule out Addison's disease.
Dr. Lam has gone through adrenal fatigue himself and recovered. Having helped thousands of adrenal fatigue sufferers recover, he has compiled together an adrenal fatigue recovery program that incorporates a whole-body approach to AFS recovery through:
While there are many nutrients that can help Adrenal Fatigue recovery, only a few are needed at any moment. Nutrients, if not dosed properly, can become toxic and make Adrenal Fatigue worse. A shotgun approach seldom works and can in fact backfire if the adrenal is not able to take in the nutrients at the right rate, time, and dose.
It is best to take it one step at a time under professional guidance to ensure the right step is taken at the proper time. This is especially true for advanced cases. Laboratory tests can be helpful, but are not critical in most cases. The key is a knowledgeable provider or nutritional coach who takes the time to understand your body with its signals and cries for help. A complete nutritional and lifestyle approach that helps the adrenal gland to normalize itself, along with ongoing adjustments in terms of nutritional supplementation to assist the adrenal during this recovery is the key. That is why with Dr. Lam's Nutritional Adrenal Fatigue Recovery Program, we provide personalized nutritional consultation with an adrenal fatigue expert to make sure your plan is individualized and correct.
Adrenal Fatigue is a decrease in the ability of the adrenal glands to carry out its normal function. The chief symptoms are fatigue, sleep disturbances, general feeling of being unwell, salt cravings, and brain fog.
Adrenal Fatigue is caused by prolonged stress from any source (including emotional, physical, mental, or environmental) that exceeds the body's capacity to adjust to the demands placed on it by stress. It is a condition that afflicts children as well as adults.
Adrenal glands can be restored to optimum health by adhering to healthy living principles. Proper rest, specific nutrition, proper supplementation, and stress reduction are key components of Adrenal Fatigue recovery. With Dr. Lam's Adrenal Fatigue Recovery Program, you can have a guide on supplement usage, beneficial exercises, diet choices, and insights from Dr. Lam's journey. You even have a personalized nutritional consultation with Dr. Lam's team to be able to ensure that you don't feel alone in this process of recovery. Empower yourself to make informed decisions and sidestep common setbacks.
Alexandraki KI, Sanpawithayakul K, Grossman A, “Adrenal Insufficiency”, In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext, South Dartmouth (MA): MDText.com, Inc, 2000, Available from: https://www.ncbi.nlm.nih.gov/books/NBK279083/
Allen, Loyd, V, “Adrenal Fatigue”, International Journal of Pharmaceutical Compounding, vol. 17, no. 1, 2013, pp. 39-44, https://pubmed.ncbi.nlm.nih.gov/23627245/
Hannibal, Kara, E, & Bishop, Mark, D, “Chronic stress, cortisol dysfunction, and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation”, Physical Therapy, vol. 94, no. 12, 2014, pp. 1816-25. https://doi.org/10.2522/ptj.20130597
{kind=link}